4 Indiana Ave Valparaiso, IN 46383
in**@*******aw.com
(219) 464-3246
You left an Indianapolis emergency room worse than when you arrived, and the hospital hasn’t explained why. Under Indiana’s Medical Malpractice Act, that’s actionable when care fell below the standard of care and caused measurable harm. Indiana’s two-year clock runs from the date of the error, not discovery, and the Medical Review Panel must precede any lawsuit.
Our Indianapolis emergency room negligence attorneys have represented Indiana malpractice victims since 1980, recovered $9.05 million in a single case, and Steven Langer is the only Indiana attorney to win ITLA Trial Lawyer of the Year twice. Call (219) 464-3246 for a free case review, no upfront fees.

An ER error is legally actionable in Indiana when the treating provider’s conduct fell below what a reasonably competent emergency physician would have done in the same situation, and that deviation directly caused measurable harm to the patient.
Not every bad outcome from emergency care is malpractice. An ER error becomes actionable under Indiana’s Medical Malpractice Act when the provider’s conduct fell below the standard of care, and that failure caused harm the patient would not have otherwise suffered.
Emergency physicians are judged against what a reasonably competent ER physician would have done facing the same clinical presentation, at the same stage, with the same information available. The standard of care accounts for time pressure and incomplete data. It does not excuse conduct that a competent physician would have recognized as inadequate.
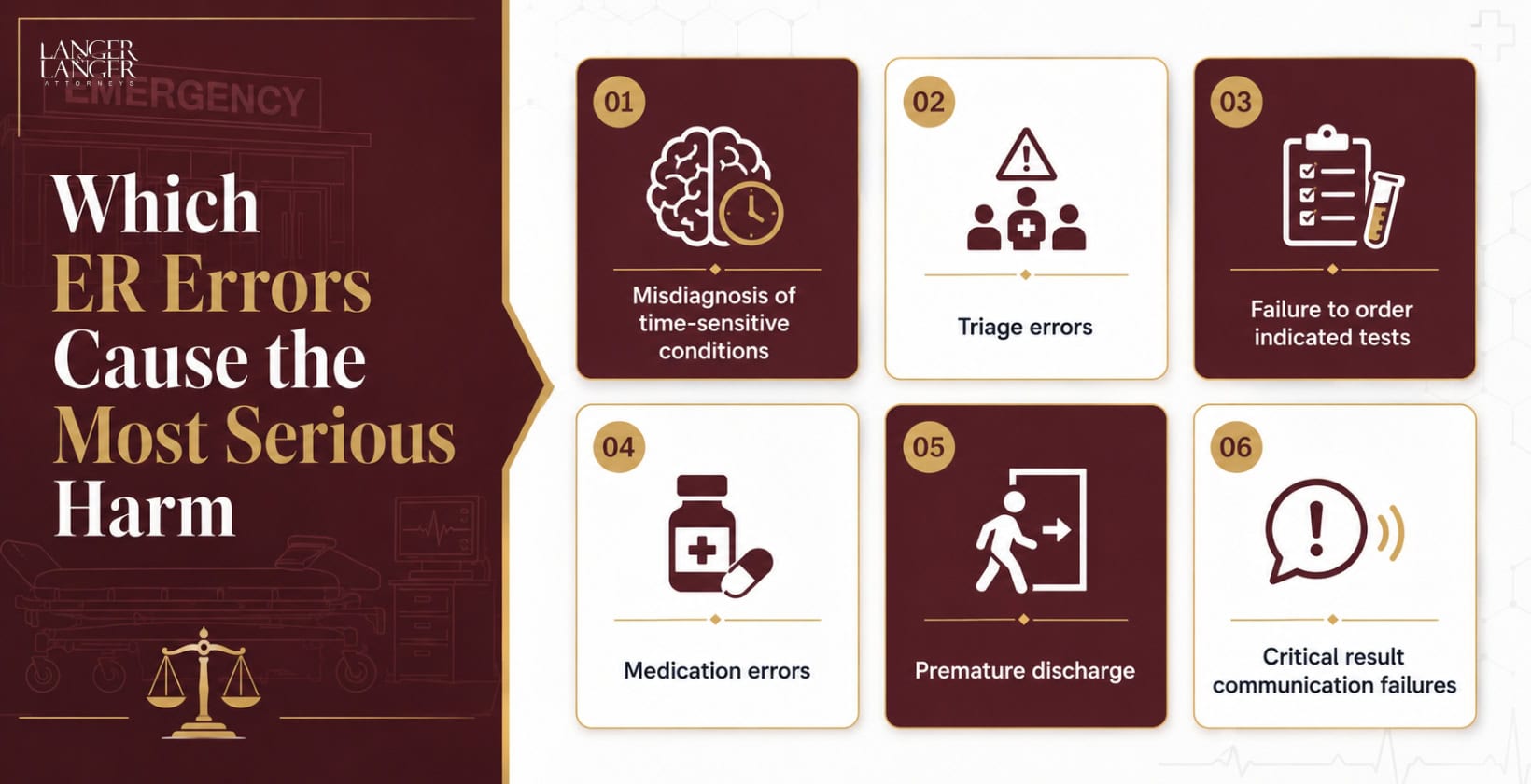
Three deviation types drive the majority of Indiana ER negligence claims:
The operative legal question: would a competent emergency physician have acted differently, and would that difference have changed this patient’s outcome?
To establish an ER negligence claim in Indiana, a patient must prove a provider-patient relationship, care below the standard of a competent ER physician, a direct causal link between that failure and the harm suffered, and concrete documented injury.
|
Element |
What It Requires |
Evidence That Supports It |
|
Duty |
A provider-patient relationship existed |
ER intake records, triage log |
|
Breach |
Care fell below the standard of a reasonably competent ER physician |
Independent expert testimony |
|
Causation |
Breach directly caused harm or reduced the probability of a better outcome |
Medical timeline, progression records, expert opinion |
|
Documented Harm |
Concrete, provable injury |
Medical bills, lost wages, treatment records |
Causation is the element that Indiana defense teams attack hardest. They argue the patient’s underlying condition, not the physician’s conduct, produced the outcome. Indiana’s Lost Chance doctrine addresses that argument directly.
Indiana adopted the Lost Chance doctrine in Mayhue v. Sparkman, 653 N.E.2d 1384 (Ind. 1995). The Indiana Supreme Court extended it in both Cahoon v. Cummings (2000) and Alexander v. Scheid (2000). When an ER error reduced the patient’s probability of a better outcome, that lost chance is compensable without proof that recovery was guaranteed.
Consider this: a patient presents with early sepsis signs, and the treating physician discharges without ordering blood cultures. The patient returns two days later in septic shock. Under the Lost Chance doctrine, the reduction in the patient’s probability of recovery is the compensable injury, and damages are proportional to the increased risk the error created.
According to Newman-Toker et al. in BMJ Quality & Safety (2024;33(2):109-120), approximately 75% of serious misdiagnosis-related harm involves vascular events, infections, and cancers. The five conditions responsible for the largest share are stroke, sepsis, pneumonia, venous thromboembolism, and lung cancer. These aren’t rare presentations. They walk into Indianapolis emergency rooms every shift.
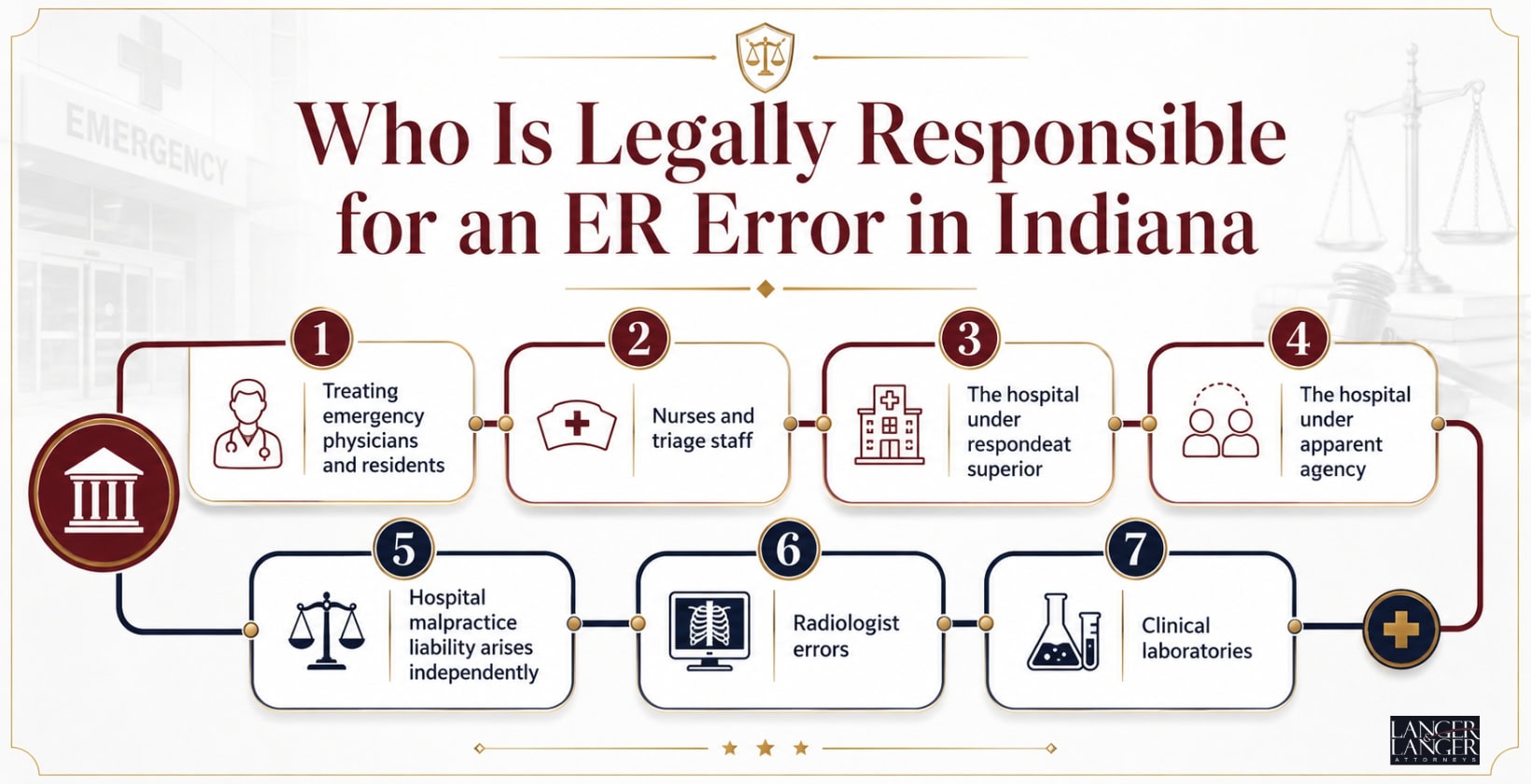
Responsibility for an Indianapolis ER error can extend beyond the treating physician to nurses, the hospital as employer and institution, contracted physician groups under the apparent agency doctrine, radiologists who misread imaging, and clinical laboratories that produced incorrect results.
Note: Eskenazi Health operates as a government entity; claims may require a separate 180-day notice of tort claim in addition to the Medical Review Panel filing.
Identifying every responsible party at the outset is the only way to access the full recovery available under Indiana law.
Indiana law mandates the Medical Review Panel before any ER negligence lawsuit can be filed. The process involves submitting a proposed complaint to the Indiana Department of Insurance, not a court, and consistently runs longer than most patients expect.
The Medical Review Panel is mandatory under IC 34-18. Three healthcare providers form the Panel, two of whom must practice in the relevant specialty, alongside one non-voting attorney chair. The Panel issues a written opinion on whether the conduct fell below the standard of care. That opinion is admissible at trial. It is not binding. A defense opinion does not end the case.
Filing the proposed complaint tolls the statute of limitations through 90 days after the claimant receives the Panel opinion under IC 34-18-7-3. The statute targets 180 days from the last panelist selection. In practice, the process runs from eight months to over a year.
We build every Panel submission to trial standards. The record the defense receives shapes how they assess and price the claim from the start.
Indiana’s statute of limitations for ER malpractice gives most victims two years from the date of the alleged error under IC 34-18-7-1. The clock is occurrence-based. It runs from when the error happened, not when the patient learned what went wrong.
A patient discharged from an Indianapolis ER in February 2024 with an undiagnosed pulmonary embolism who pieces together the full picture in February 2026 may already be time-barred. The discovery rule applies only where no reasonable person could have identified the error within two years. Indiana courts apply that exception sparingly.
One exception applies to minor patients: a child under age six at the time of the malpractice has until their eighth birthday to file.
The Medical Review Panel must be completed before any court filing. Retaining counsel, gathering records, engaging an expert, and submitting a complete Panel file must all happen within a window shorter than the statutory period alone suggests. Waiting a year to call an attorney may leave weeks, not months, to build a viable submission.
An Indianapolis ER negligence claim can produce economic damages for medical costs, lost wages, and future care, and non-economic damages for pain, emotional harm, and loss of function. Indiana’s cap under IC 34-18-14-3 sets a total recovery ceiling of $1,800,000 for malpractice after June 30, 2019.
Economic damages may include:
Non-economic damages may include:
The provider’s insurer covers the first $500,000. The Indiana Patient’s Compensation Fund (PCF) covers up to $1,300,000 above that limit. The cap applies to qualified healthcare providers under Indiana law and covers the combined total of economic and non-economic damages.
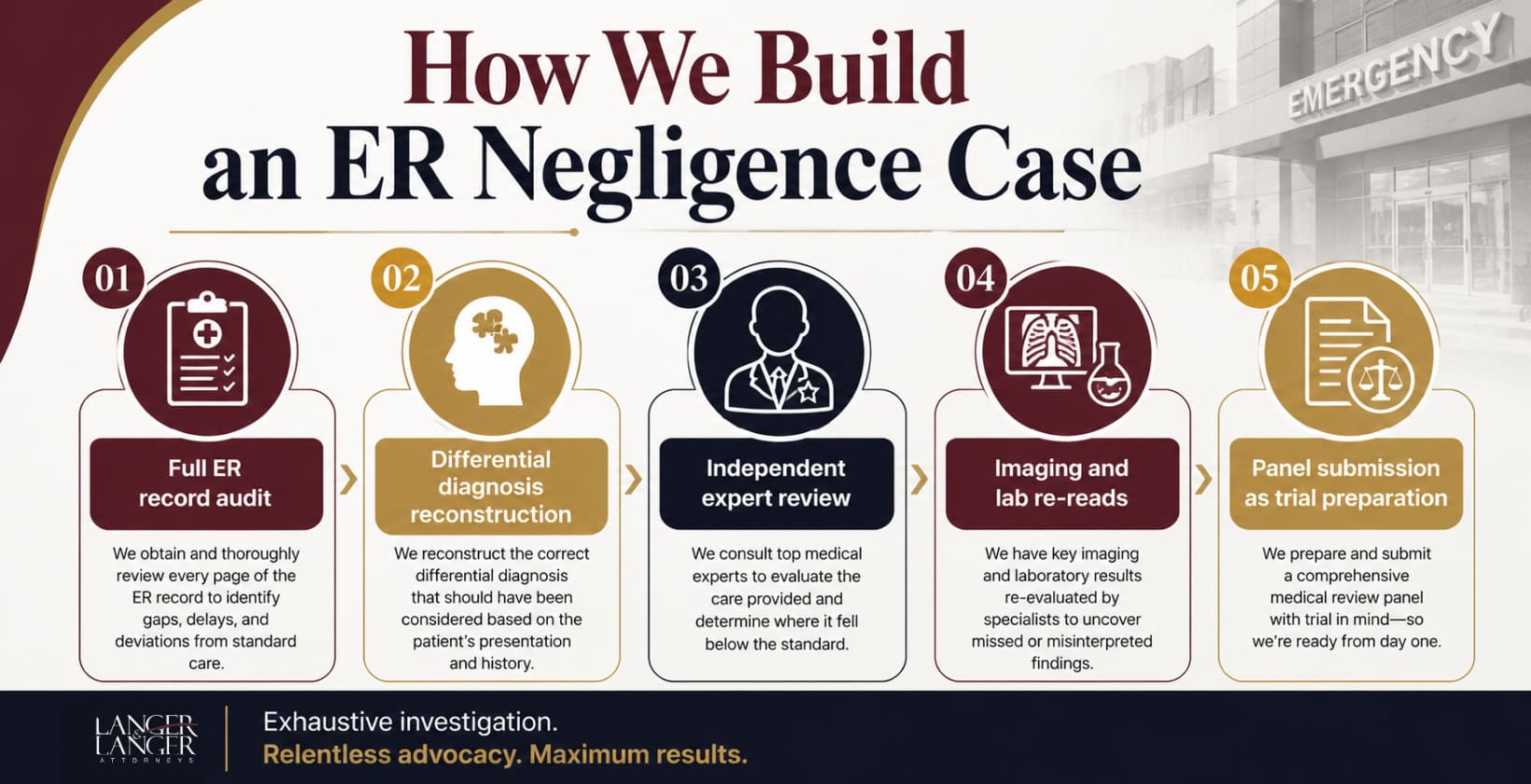
We reconstruct the clinical picture through five parallel tracks: a full ER record audit, differential diagnosis reconstruction, independent expert review, imaging and lab re-reads, and a Panel submission built to trial standards from the start.
That level of preparation is visible to opposing counsel at every stage and affects how cases resolve before trial.
Steven L. Langer is the only Indiana attorney to win ITLA Trial Lawyer of the Year twice (2004 and 2009). He serves as Indiana State Chair of the American College of Trial Lawyers, previously served as ITLA President, and earned Best Lawyers: Lawyer of the Year 2024 for personal injury litigation. AV Preeminent rated. Published author on Indiana’s Medical Malpractice Act.
Our team:
Our results in Indiana medical malpractice:
We prepare every ER negligence case for trial from the first file review. Opposing counsel recognizes that posture, and it shapes outcomes before any courtroom appearance.
Past results do not guarantee any future outcome. Every case is different.
We serve individuals and families across the entire state of Indiana. Our main office is located at 4 Indiana Ave, Valparaiso, IN 46383, and we handle medical malpractice claims arising from care provided in hospitals, clinics, and outpatient settings across the state.
We represent clients in communities including:


It may mean the ER committed premature discharge. If your condition was present or developing at your visit and a competent physician would have identified it, sending you home can establish breach and causation under Indiana's Medical Malpractice Act.
The hospital may still be liable under Indiana's apparent agency doctrine. If you reasonably believed the ER physician was a hospital employee, the institution can be held liable even if that physician was contracted through an independent group.
The case can still proceed. A Panel opinion favoring the defense is admissible at trial but is not binding. Indiana courts have confirmed that a plaintiff may pursue a malpractice claim regardless of the Panel's conclusion.
Indiana's statute of limitations is two years from the date of the error, not discovery. Because the Medical Review Panel must precede court filing and the process alone runs eight months to over a year, your practical window to retain counsel is shorter than two years.
It depends on whether a competent ER physician facing the same presentation would have acted differently. An independent emergency medicine expert reviews the record and differential diagnosis of the symptoms required. That review determines whether the conduct fell below the standard of care.
Under IC 34-18-14-3, maximum recovery is capped at $1,800,000 for malpractice after June 30, 2019. The provider's insurer covers the first $500,000. The Patient's Compensation Fund covers up to $1,300,000; beyond that. Actual recovery depends on documented harm.
Under IC 34-51-2, Indiana reduces your damages proportionally if your own conduct contributed to the harm, and bars recovery entirely if you are found more than 50% at fault. This is a standard defense in ER negligence cases and must be addressed from the Panel submission forward.
Indiana’s two-year deadline runs from the date of the error, not the date you understood what went wrong. The Medical Review Panel must be completed before any lawsuit can be filed, and that process alone runs eight months to over a year, making your actual window shorter than most patients realize. The earlier we review the ER record, the more your options and evidence are preserved.
After your consultation, Langer & Langer requests the complete ER record, engages an independent emergency medicine expert, and gives you a direct assessment of claim viability before any commitment is required.
(219) 464-3246 4 Indiana Ave, Valparaiso, IN 46383
Medical errors are complex. We cut through the confusion – just share your records and our team will give you an honest case evaluation, free of charge.
© 1980-2026 Langer & Langer • All Rights Reserved
Copyright © 1980-2026 All Rights Reserved.
Past results do not guarantee any future outcome, and every case is different.
We improve our products and advertising by using Microsoft Clarity to see how you use our website. By using our site, you agree that we and Microsoft can collect and use this data.
Have legal questions or need expert advice? Our experienced team is here to help.
Langer and Langer
Accessibility Statement
Compliance status
We firmly believe that the internet should be available and accessible to anyone, and are committed to providing a website that is accessible to the widest possible audience, regardless of circumstance and ability.
To fulfill this, we aim to adhere as strictly as possible to the World Wide Web Consortium’s (W3C) Web Content Accessibility Guidelines 2.1 (WCAG 2.1) at the AA level. These guidelines explain how to make web content accessible to people with a wide array of disabilities. Complying with those guidelines helps us ensure that the website is accessible to all people: blind people, people with motor impairments, visual impairment, cognitive disabilities, and more.
This website utilizes various technologies that are meant to make it as accessible as possible at all times. We utilize an accessibility interface that allows persons with specific disabilities to adjust the website’s UI (user interface) and design it to their personal needs.
Additionally, the website utilizes an AI-based application that runs in the background and optimizes its accessibility level constantly. This application remediates the website’s HTML, adapts Its functionality and behavior for screen-readers used by the blind users, and for keyboard functions used by individuals with motor impairments.
If you’ve found a malfunction or have ideas for improvement, we’ll be happy to hear from you. You can reach out to the website’s operators by using the following email
Screen-reader and keyboard navigation
Our website implements the ARIA attributes (Accessible Rich Internet Applications) technique, alongside various different behavioral changes, to ensure blind users visiting with screen-readers are able to read, comprehend, and enjoy the website’s functions. As soon as a user with a screen-reader enters your site, they immediately receive a prompt to enter the Screen-Reader Profile so they can browse and operate your site effectively. Here’s how our website covers some of the most important screen-reader requirements, alongside console screenshots of code examples:
Screen-reader optimization: we run a background process that learns the website’s components from top to bottom, to ensure ongoing compliance even when updating the website. In this process, we provide screen-readers with meaningful data using the ARIA set of attributes. For example, we provide accurate form labels; descriptions for actionable icons (social media icons, search icons, cart icons, etc.); validation guidance for form inputs; element roles such as buttons, menus, modal dialogues (popups), and others. Additionally, the background process scans all the website’s images and provides an accurate and meaningful image-object-recognition-based description as an ALT (alternate text) tag for images that are not described. It will also extract texts that are embedded within the image, using an OCR (optical character recognition) technology. To turn on screen-reader adjustments at any time, users need only to press the Alt+1 keyboard combination. Screen-reader users also get automatic announcements to turn the Screen-reader mode on as soon as they enter the website.
These adjustments are compatible with all popular screen readers, including JAWS and NVDA.
Keyboard navigation optimization: The background process also adjusts the website’s HTML, and adds various behaviors using JavaScript code to make the website operable by the keyboard. This includes the ability to navigate the website using the Tab and Shift+Tab keys, operate dropdowns with the arrow keys, close them with Esc, trigger buttons and links using the Enter key, navigate between radio and checkbox elements using the arrow keys, and fill them in with the Spacebar or Enter key.Additionally, keyboard users will find quick-navigation and content-skip menus, available at any time by clicking Alt+1, or as the first elements of the site while navigating with the keyboard. The background process also handles triggered popups by moving the keyboard focus towards them as soon as they appear, and not allow the focus drift outside it.
Users can also use shortcuts such as “M” (menus), “H” (headings), “F” (forms), “B” (buttons), and “G” (graphics) to jump to specific elements.
Disability profiles supported in our website
Additional UI, design, and readability adjustments
Browser and assistive technology compatibility
We aim to support the widest array of browsers and assistive technologies as possible, so our users can choose the best fitting tools for them, with as few limitations as possible. Therefore, we have worked very hard to be able to support all major systems that comprise over 95% of the user market share including Google Chrome, Mozilla Firefox, Apple Safari, Opera and Microsoft Edge, JAWS and NVDA (screen readers).
Notes, comments, and feedback
Despite our very best efforts to allow anybody to adjust the website to their needs. There may still be pages or sections that are not fully accessible, are in the process of becoming accessible, or are lacking an adequate technological solution to make them accessible. Still, we are continually improving our accessibility, adding, updating and improving its options and features, and developing and adopting new technologies. All this is meant to reach the optimal level of accessibility, following technological advancements. For any assistance, please reach out to