Yes. You can sue a hospital for misdiagnosis in Indiana when a diagnostic error caused measurable harm under Indiana’s Medical Malpractice Act (MMA). A valid claim requires four elements: a provider-patient relationship, a diagnosis below the standard a reasonably careful provider would have met, proof that the failure caused injury, and documented harm. Both the treating provider and the hospital can carry liability.
Indiana’s process requires a proposed complaint filed with the Indiana Department of Insurance (IDOI) and reviewed by a medical review panel (MRP) before any court filing. The two-year deadline under Indiana Code (IC) 34-18-7-1 runs from the date of the error. Total recovery is capped at $1.8 million under IC 34-18-14-3.
Key Takeaways
- A valid claim requires duty, breach, causation, and documented harm. All four are required.
- Hospitals face liability through vicarious liability and the apparent agency doctrine, not only individual providers.
- A proposed complaint must be filed with the IDOI before any court filing.
- Indiana is an occurrence-based state: the two-year deadline under IC 34-18-7-1 starts on the date of the error, not the date of discovery.
- Total recovery is capped at $1.8 million for acts after June 30, 2019, under IC 34-18-14-3.
- The PCF covers amounts above the provider’s $500,000 liability, up to $1.3 million.
What Qualifies as Misdiagnosis Under Indiana Law
A misdiagnosis occurs when a healthcare provider fails to correctly identify a patient’s condition. It takes three forms:
- A wrong condition is identified, and the patient receives treatment for an illness they do not have.
- A diagnosable condition goes completely undetected, and no diagnosis is made.
- A correct condition is identified so late that the delay itself constitutes the harm.
Not every wrong diagnosis is malpractice. Indiana courts evaluate whether the error fell below what a reasonably careful provider in the same specialty would have done, not simply whether the outcome was bad.
Misdiagnosis vs. Failure to Diagnose
| Category | Misdiagnosis | Failure to Diagnose |
| What Happened | Wrong condition identified | No condition identified |
| Treatment Path | Patient treated for an illness they did not have | No treatment was initiated for the actual condition |
| How Condition Advanced | Worsened while incorrect treatment was given | Worsened without any intervention |
| Causation Focus | Harm from the incorrect treatment path | Harm from the absence of timely treatment |
| Supports Indiana MMA Claim | Yes | Yes |
Both support an Indiana medical malpractice claim. The causation argument differs between them, which shapes the evidence required and how the claim is built.
Four Legal Elements Indiana Courts Require
All four elements must be present. A claim that satisfies three but fails on the fourth does not proceed regardless of how clear the error appears in the record.
Duty of Care
A provider-patient relationship must have existed at the time of the diagnostic error. In a hospital setting, this is established the moment a patient is admitted, registers at an emergency room (ER), or checks in at a clinic. That registration record, intake form, or admission paperwork is itself the proof. Once that relationship exists, the provider owes the patient a duty to meet the applicable standard of care. This element is rarely contested in misdiagnosis cases. It is the baseline from which every other element flows.
Breach of the Standard of Care
Breach means the provider’s diagnostic decision fell below what a reasonably careful provider in the same specialty would have done. Indiana law requires a qualified medical expert to testify on what the standard required and where it was violated. The three most common failure patterns are failure to order indicated tests, misreading imaging results, and dismissing documented symptoms without follow-up.
Causation and the Lost Chance Doctrine
The diagnostic error must have directly caused measurable harm. A breach with no resulting injury does not support a claim.
Indiana courts allow recovery under the increased risk of harm framework established in Mayhue v. Sparkman (1995) and developed in Cahoon v. Cummings and Alexander v. Scheid (both 2000). If a provider’s negligence worsened the patient’s position, a claim may proceed. A cancer patient whose survival probability dropped from 70% to 30% because of a diagnostic delay has suffered a concrete, provable injury. This element is the most contested, and where expert medical testimony carries the most weight.
Documented Harm
Concrete, provable injury is required: additional procedures, a worsened prognosis, extended recovery, financial losses from added medical costs or missed work, or a documented reduction in quality of life. Harm is not implied from the error. It must be established with evidence, and without it, the claim does not proceed.
When the Hospital Carries Legal Liability
Indiana patients can sue the hospital as an institution, not only the individual provider who made the error. Three distinct theories can each attach liability to the hospital independently.
Vicarious Liability for Employed Providers
When the negligent provider is a direct hospital employee, the hospital is liable under respondeat superior. ER physicians, radiologists, and hospitalists are frequently employed directly by the hospital, making this the most common path to institutional liability in misdiagnosis cases.
Apparent Agency and Independent Contractors
Many hospitals contract with physician groups rather than employing physicians directly. Indiana courts apply the apparent agency doctrine: if the hospital held the provider out as part of its staff through admissions paperwork, signage, or patient-facing communications, the hospital can be held liable even when the provider was technically an independent contractor. Patients have no reliable way to distinguish the two in most settings.
Standalone Institutional Failures
A hospital can carry independent liability separate from any individual provider’s conduct. Inadequate credentialing, failure to maintain diagnostic equipment, deficient protocols for flagging abnormal test results, and systemic communication failures between departments each constitute institutional negligence without requiring proof that a specific physician acted below the standard of care.

Conditions Most Often Involved in Indiana Misdiagnosis Cases
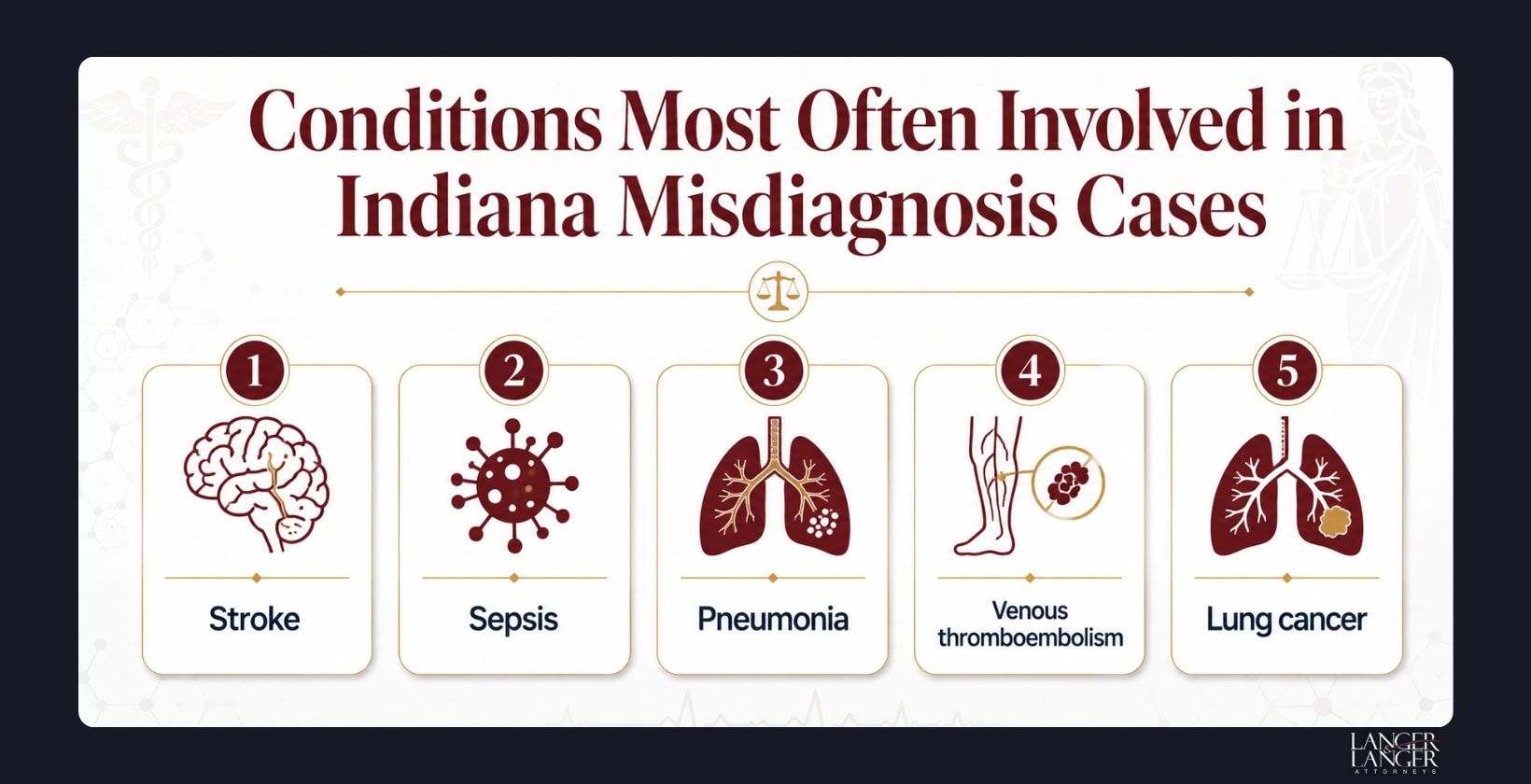
Research from Newman-Toker et al. (BMJ Quality & Safety, January 2024, PubMed/NIH) found that approximately 75.8% of all serious misdiagnosis-related harms involve vascular events, infections, and cancers. Five conditions account for 38.7% of those harms:
- Stroke: Younger patients and those presenting with dizziness rather than limb weakness face the highest misdiagnosis rates. Every minute without treatment advances irreversible brain injury.
- Sepsis: Deteriorates rapidly when unrecognized. A patient discharged with signs of infection can enter septic shock within hours.
- Pneumonia: Frequently misidentified in older patients. Delayed antibiotic treatment allows infection to advance toward respiratory failure.
- Venous thromboembolism: Routinely missed in emergency settings. A blood clot that travels to the lungs can be fatal within hours of an incorrect diagnosis.
- Lung cancer: A missed finding on a chest imaging study can move a patient from a stage where curative treatment is available to one where it is not.
Evidence That Supports a Misdiagnosis Claim in Indiana
A qualified medical expert is required under Indiana law to testify on the standard of care and where it was violated. Beyond expert testimony, strong cases rely on:
- Medical records: Physician notes, imaging reports, lab results, pathology reports, and the test-ordering timeline establish what the provider knew and when.
- Personal documentation: Every appointment, every symptom reported, and every instruction given or withheld, written while details are still clear.
- Financial records: Medical bills, wage loss records, and costs of all additional treatment required because of the misdiagnosis.
The strongest cases show a clear, documented gap between what the records indicate the provider knew and what action was actually taken.
Indiana’s Medical Review Panel: A Required Step Before Court
Under IC 34-18, no misdiagnosis lawsuit seeking more than $15,000 can be filed in an Indiana court without first completing the MRP process. A court filing made without it will be dismissed.
Filing a proposed complaint with the IDOI initiates the process. The panel consists of three healthcare providers, with two required to practice in the relevant specialty under IC 34-18-10-8, and one non-voting attorney chair under IC 34-18-10-3. The panel issues a written opinion on whether the conduct fell below the standard of care. That opinion is admissible at trial but not binding. The process typically runs eight months to over a year. Filing the proposed complaint also tolls the statute of limitations through 90 days after the claimant receives the panel’s opinion under IC 34-18-7-3.
Indiana’s Filing Deadline: Why the Clock Starts Earlier Than Most Patients Expect
Indiana is an occurrence-based state. Under IC 34-18-7-1, the two-year deadline starts on the date the error occurred, not the date it was discovered. A patient misdiagnosed in January 2024 who does not discover the error until January 2026 is already time-barred.
Two exceptions apply. The discovery rule covers narrow circumstances where no reasonable person could have discovered the malpractice within the two-year window, but it is litigated case by case and does not automatically extend the deadline. A child under six at the time of the alleged malpractice has until their eighth birthday to file. Minors six and older follow the standard two-year deadline.
Compensation Available and Indiana’s Damages Cap
A successful claim can recover added medical costs, future treatment expenses, lost income, pain and suffering, emotional distress, and loss of quality of life. Wrongful death claims arising from medical malpractice are subject to the same $1.8 million cap under the MMA.
Under IC 34-18-14-3, total recovery for acts after June 30, 2019, is capped at $1.8 million, whether the case settles or goes to verdict. The healthcare provider’s insurer covers the first $500,000. The PCF, administered by the IDOI, covers the remaining balance up to $1.3 million.
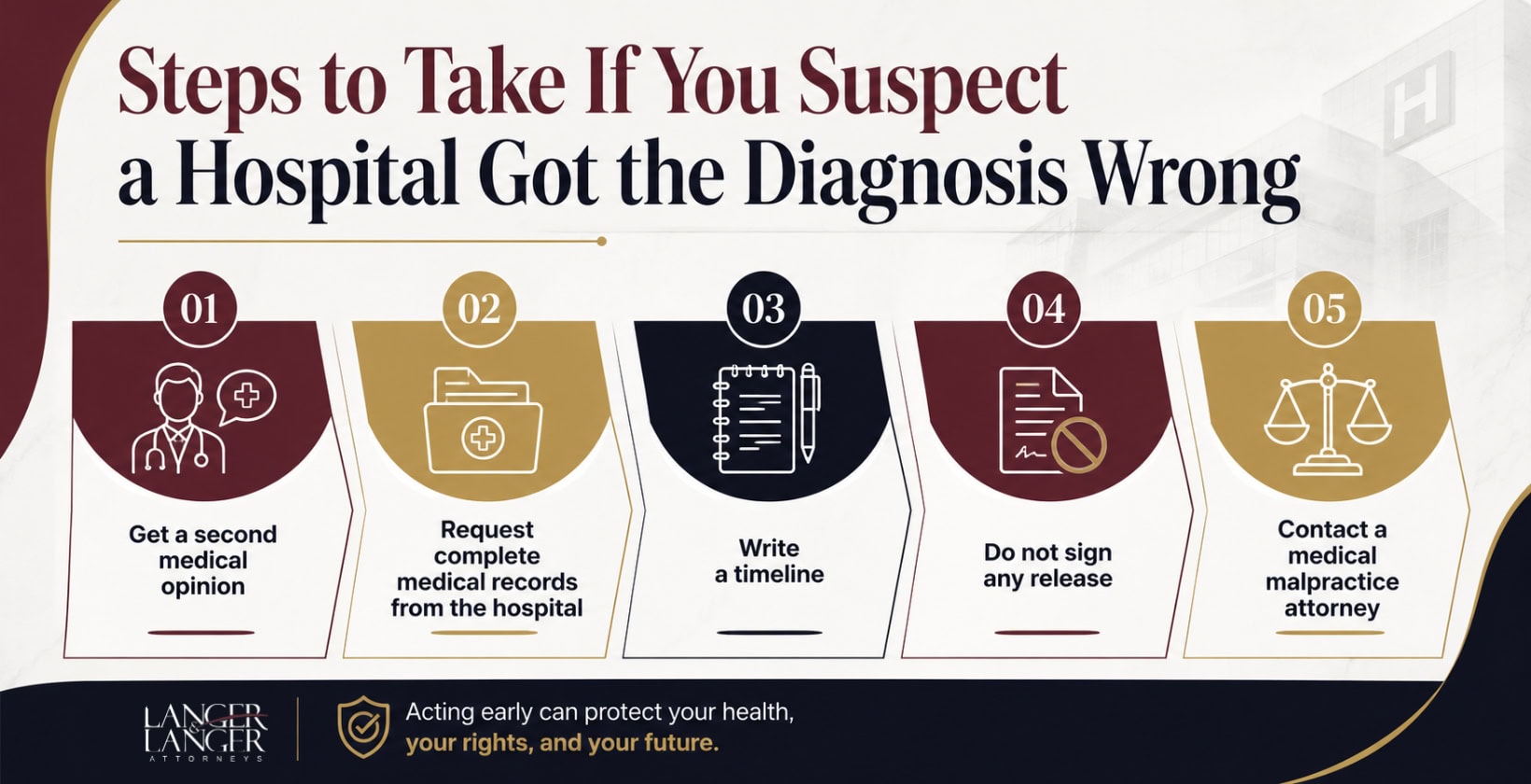
Steps to Take If You Suspect a Hospital Got the Diagnosis Wrong
Taking the right steps early protects both your health and your legal options.
- Get a second medical opinion immediately and start a new documented treatment record.
- Request complete medical records from the hospital, including the discharge summary, imaging reports, lab results, and physician notes. You have a legal right to those records.
- Write a timeline of every appointment, every symptom reported, and every instruction given or withheld while details are still clear.
- Do not sign any release or accept any payment from the hospital or its insurer before speaking with an attorney. Signing closes the claim permanently.
- Contact a medical malpractice attorney before the two-year deadline under IC 34-18-7-1 closes.
Talk with an Indiana Medical Malpractice Attorney
Langer & Langer has represented Indiana medical malpractice clients since 1980. The firm has secured 18 verdicts and settlements exceeding $1 million. The firm reviews Indiana misdiagnosis claims, works with qualified medical experts to evaluate the standard of care, and handles the proposed complaint and MRP process under the MMA.
Call 219-464-3246 or visit 4 Indiana Ave, Valparaiso, IN 46383 to request a free case review.